


COVID-19 on the Frontlines: Lessons from Law Enforcement in Amravati, India
By Harssh A Poddar, assisted by Tarun Krishnakumar
The second wave of the pandemic in India, caused by the Delta variant, caught global attention and brought unparalleled hardship and suffering to India – leading to over 200,000 deaths between March and June 2021. In early August this year, the country reported weekly rises in case rates for the first time since May, foreshadowing a third wave of outbreaks. Even as the pandemic ravaged economies and communities, work-from-home quickly became routine for large sections of society. The “new normal” emerged as an enduring cliché to describe the status quo. However, as much as things changed for many, the more they stayed the same for some. In India, frontline workers (FLWs) were not only required to continue their usual responsibilities but also found their task load exponentially increased as cases surged across the country.
While the selfless sacrifices of healthcare workers are rightly acknowledged, the steadfast contributions of law enforcement are sometimes overlooked. In the Indian context, law enforcement –i.e., police and paramilitary forces—faced unique and unprecedented challenges during the pandemic. They were required to enforce what was likely the world’s most stringent lockdown all while securing India’s vast State elections. The particular unit that I command, the 9th battalion of the State Reserve Police Force (SRPF), is located in Amravati, a city where the Delta mutation was first detected and is widely acknowledged as the starting point of the second wave.
Headquartered in the epicenter of the pandemic, the personnel of the battalion faced heightened risk being deployed across India for a variety of tasks such as deployment to prevent electoral violence and malpractice in the state of Uttar Pradesh, India’s largest state, to combating armed non-state actors in the jungles of central India. The criticality of these duties places unique emphasis on the need for a methodical approach in managing law enforcement exposure to the pandemic. This unit, consisting of over 1100 personnel and 3000 family members, was successful in doing so because it did not report a single death due to COVID-19 during the second wave that surged through India.
Improving Vaccine Awareness
The primary step in limiting law enforcement exposure was a concerted effort to improve inoculation levels of all personnel who were eligible to receive vaccination.
While strategic management of infrastructure, including vaccine distribution, were integral to the successful response, their effect might have been limited by a widely-prevalent vaccine hesitancy or lack of awareness. Therefore, a critical first step was to establish reliable and trusted channels of information flow to ensure that information asymmetries or misconceptions around the vaccines were effectively addressed by health personnel. SRPF organized as many as ten awareness sessions for service members, achieving 97 percent coverage of personnel and their families. These were followed by dedicated vaccination camps for SRPF personnel and their eligible family members.
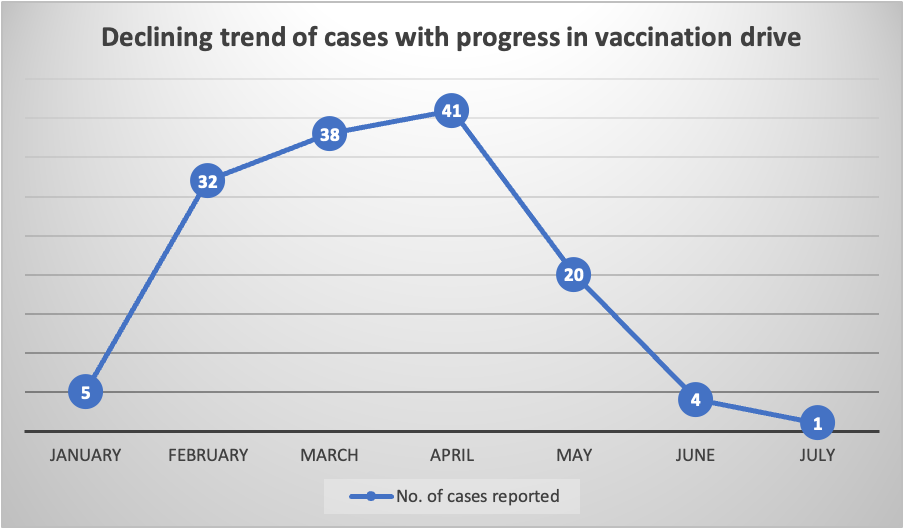
These efforts proved to be fruitful with 100 percent first dose vaccination of personnel being achieved within a span of four weeks starting from February 2, when vaccination of FLWs commenced in India and 92 percent second dose coverage by May. The sharp impact of the vaccination drive in reducing cases in the battalion is illustrated by the graph below:
Infection Management and Critical Care
While vaccination is key to resilience, breakthrough cases cannot be avoided and must be actively anticipated. At SRPF, a rigorous process of testing based on exposure and symptoms was instituted – with isolation facilities readily on hand for those testing positive. More than 1600 screening tests were conducted in a period of three months.
For personnel who tested positive, the priority was to monitor for signs of sudden deterioration and anticipation of critical care needs. Here, based on medical inputs, a rigorous monitoring regime was instituted to track vital functions and precursor signs of deterioration including:
(i) The institution of a scanning regime to track the onset of pneumonia (or pulmonary infections) in patients. Studies have shown that scans may offer valuable insights around the severity of infection and help in definitive prognosis.
(ii) Testing for markers which studies have shown to be “highly predictive” of the onset of cytokine storm and the need for mechanical ventilation.
(iii) Testing to track blood clotting that may cause cardiac arrest due to pulmonary thromboembolism. Studies have shown that certain tests are predictive of “serious illness and death” relating to COVID-19 and can provide valuable assistance in triaging patients.
(iv) Kidney and Liver Function Tests to monitor organ functions and help assess risk for multi-organ failure in patients.
(v) In addition, measures were instituted to ensure regular monitoring of oxygen levels which can aid in early detection of hypoxia and help triage timely, higher-level care.
These measures ensured that rapid deterioration in patient conditions did not catch health workers off-guard, and treatment could be prioritized to those at highest-risk. To be sure, SRPF’s successful vaccination campaign ensured that critical care facilities were never overwhelmed— there were no more than 25 patients at any given point in time.
Risk-based Approach to Quarantine and Isolation
These preventative and treatment strategies were accompanied by a stringent and graded approach to quarantining officers and families based on risk due to travel or exposure. In addition, access to the SRPF base, spread over 300 acres, was tightly controlled with groceries and other essentials being provided to residents via home delivery.
Before being allowed to return to base, officers returning from external deployments were quarantined off-base for a period of 5 days before being tested (Level 1 Quarantine). Anyone testing positive was moved to institutional quarantine in a separate part of the base (Level 2 Quarantine). Lastly, family members who had been in close contact with those who tested positive were moved to a separate family institutional quarantine for a period of 3 days before being tested (Level 3 Quarantine).
These measures proved effective particularly in a scenario where housing in the cantonment is clustered together in close proximity.
Strategic Planning: A Necessity
As the above instances illustrate, law enforcement exposure to the pandemic can be managed through early strategic planning, preparedness measures, and early procurement. The SRPF hospital managed to acquire two oxygen concentrators to support patients much before widespread scarcity took hold of the commercial market. These were critical in supporting high-risk patients pending transfer to hospitals having oxygenated beds available. This two-tiered approach to on-base medical care helped ensure a risk-based approach to treatment while also ensuring minimal dependency on the overwhelmed local health system except in exigent cases.
At the same time, also essential was coordination and partnership by SRPF with off-base public health authorities on an ongoing basis. Instances of this close cooperation included: the organization of vaccination camps for SRPF personnel and their families, advice from local authorities on the creation of micro containment zones on base, as well the provision of testing and tele-medicine facilities for quarantined personnel. Beyond local public health authorities, SRPF also coordinated with private diagnostic service providers to conduct some of the proactive monitoring detailed above. These partnerships go to show the need for law enforcement stakeholders to carefully assess their capabilities and seek external support to supplement them.
It is also crucial that law enforcement leadership adheres to a two-layered model of data analysis and supervision. At the macro-level, it is vital that policies relating to vaccination, quarantine, exposure risk during deployment are founded on empirical data analysis and are relentlessly implemented. However, given that medical science is yet to fully comprehend the vagaries of COVID-19 infection, each case must also be monitored at the individual level and medical amenities must be made available as per requirement.
In situations where health resources are on the verge of being overwhelmed, the key to success lies in advance planning and preparedness that can counter the devastating effects of the virus.
A photo series of this piece can be found here.

Harssh A Poddar is an officer of the 2013 batch of the coveted Indian Police Service (IPS). He has served at the helm of law and order maintenance in some of the most testing jurisdictions of India. His initiatives on de-radicalization, service reform at police stations, countering fake news and electoral management have received honors at the national level. He was rated among the most impactful civil servants of India in 2019.
The work done by his team in the first wave of the pandemic was published as a best practice in pandemic policing by the Ministry of Home Affairs, Government of India.
Prior to joining the IPS, he graduated with a masters degree in law from the University of Oxford as a Chevening Scholar and was working as a corporate lawyer with Clifford Chance LLP in London.
Cover photo is provided by the author.




